
This article is the second of three reflections on community health workers. The first post is here, and it introduced the general concept of what health workers can do. It generally drew on The WHO guideline on health policy and system support to optimize community health worker programs.
This post imagines what might be happening in our community today, if we had community health workers already in place to work with individuals who have been living without housing.
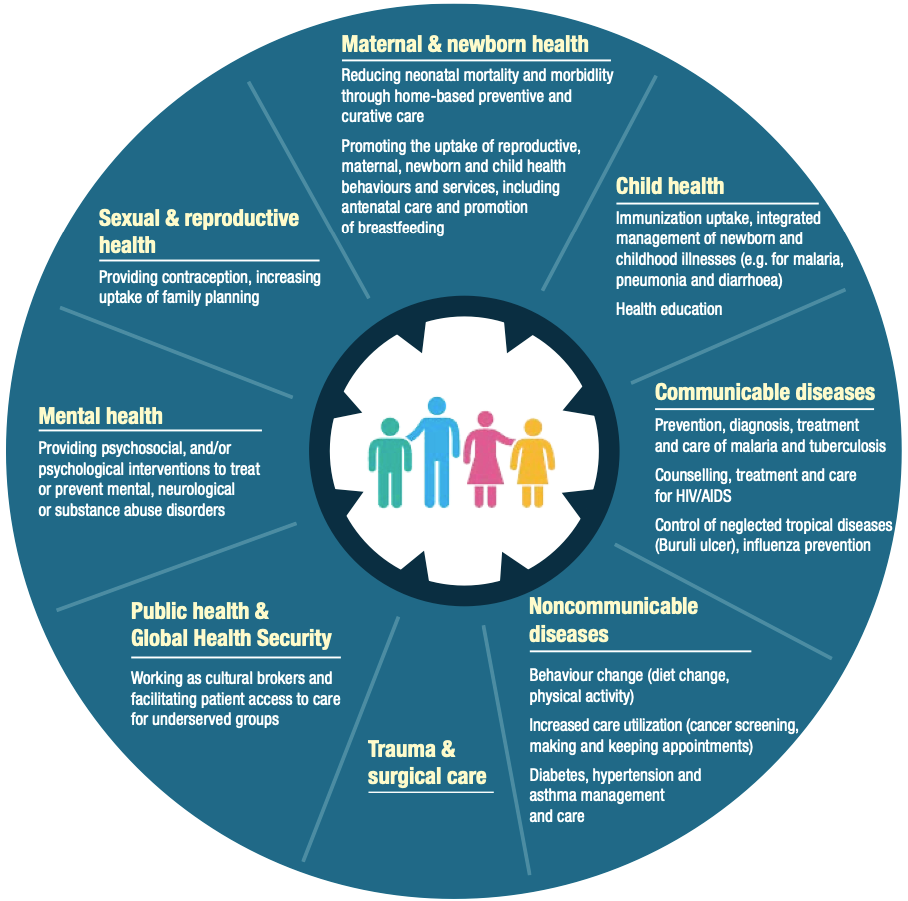
The following diagram from the WHO guidelines lays out the variety of primary healthcare services for which there is some evidence of community health worker effectiveness.

Note how varied they are. They include mental health–something that afflicts 50% or more of chronically homeless individuals. They also include communicable diseases and the idea of acting as “cultural brokers” to facilitate care for underserved groups. Finally, they include behavior change efforts to encourage people to adopt healthier behaviors.
Now imagine we had already put into place, before the current COVID-19 crisis, a system of community health workers, let’s call them community navigators, whose job was to build relationships with homeless individuals, help them connect to legal, and social services, and become people of trust with them.
Such workers would already be a vital connecting point to encourage people struggling to find housing to enter our local temporary voucher program until they could find permanent housing. They would assure that homeless individuals with chronic illnesses would have access to and use medications. They could ensure they kept appointments for legal or other issues. The navigators could be general “connectors” to help bring homeless people back into the community. These individuals would be trusted people.
In such a situation, when COVID-19 strikes, these people would provide rapid feedback on the needs and likely risk factors of the people with whom they have been working.
In the case of California and Yolo County, which have implemented temporary emergency housing for at-risk homeless people in hotels, they could help determine which of their contacts met risk criteria and rapidly connect them to the program. Further, they could visit (by phone or at a safe distance), these people every day or so and encourage them to protect themselves, provide needed medication, and be friends in a lonely time.
If one of their contacts contracted, or was a contact of a person who contracted the virus, they could reach out to them, help them move into isolation or quarantine, and then support them to maintain that status until it was safe to leave.
I raise this example because we have talked about implementing a “navigator” program in Davis. We believe that we have the volunteers who would participate, and we have discussed a recruitment and training strategy.
The point is that once we invest in community health workers for particular purposes, we can mobilize them in times of crisis, or for other related needs in the community. They become a permanent community asset–not just essential components of our social capital, but also critical rapid action resources within our healthcare infrastructure.
In the next and final installment on community health workers, I will examine their role in the movement to “defund the police.”
